ISSN: 1204-5357
ISSN: 1204-5357
By Harshavardhan Halve, Professor, Intitute of Management Technology, Nagpur and Vikrant
Kulkarni, Student Manager, Institute of Management Technology, Nagpur
Email: halveharsh@hotmail.com , kulkarni.kulkarni@gmail.com
Dr. Harshavardhan Halve, has more then 12 years of Teaching experience of Computer Science & Information Technology to both Management & Technical streams. Being a Master Of Science (Mathematics with specialization in Operations Research), P.G. Diploma in Systems Management, Post Graduate Diploma in Computer Application and PhD in Information Systems He has keen interest in the area of Computer based optimization techniques in Business. He worked for Jabalpur University & a Local college for 11 years & then worked in S. P. Jain Institute of Management & Research, Mumbai. He has provided consultancy to various organizations for I.T. Infrastructure Setup & Management and ELearning. He has published articles in national seminars & national Journals in the area of Information Technology & Management. DR. Harshvardhan Halve is the member of faculty council of Department Of Maths & Computer Science, Rani Durgawati V.V., Jabalpur and also member of Board of Studies in two Autonomous Colleges of Higher Education. He is on the Board of Examiners of RDVV, Jabalpur for MCA, MBA & IT related courses in the university. He is a registered Counselor of Indira Ghandhi National University for MBA & MCA courses. He is also approved Project guide & examiner for the same University. He is currently working as a Professor for Information Systems in I.T Department of Institute of Management Technology, Nagpur.
Vikrant Kulkarni, is pursuing his MBA from Institute of Management Technology, Nagpur. He has completed his Bachelor of Engineering in Electronics and Telecommunication from Maharashtra Institute of Technology, Pune. After that he was working with TATA CONSULTANCY SERVICES LTD. for one year for client General Electric. Interested in learning the managerial aspects of whatever that comes across. He has won numerous National Level Prizes for the project on Face and Speech Recognition. He has also presented papers in National Seminars and Seminars conducted by IEEE.
Visit for more related articles at Journal of Internet Banking and Commerce
The development of healthcare facilities is only not influenced by the opening of healthcare centers and hospitals but more so by their effective administration and value-orientation. If hospitals or the healthcare centers are well managed we canôÃâ¬Ã³Ã¦t deny quantitative-cumqualitative improvement in the healthcare services. The scope of service now includes health care guidance, preventive care, post clinical attention, care and advice. Hospitals may handle a person who is not a patient and hence we call a person visiting a hospital a customer and not a patient. Like any other business, the management of hospitals has changed from an art to a science and then to a technology. TodayôÃâ¬Ã³Ã¦s hospitals use a lot of medical hardware and software in health care activity. Health care decisions are based on diagnostic aids and assistance through an X-ray, scanning, pathological tests, and knowledge base of case history, etc. the operational aspect of the health care is supported by a lot of equipment and instrument specially developed for the purpose. The role played by these aids is so vital and important that it is called medical engineering. The medical engineering has helped the medical professionals to reduce the drudgery of health care and concentrate on diagnosis, prescriptions and treatment. The management of the infrastructure of equipment, instruments, etc. is very important management function supporting the effect of offering a distinctive service to the customer.
In hospitals there are critical resources such as an operation Theatre, an X-ray lab, hospital beds, etc. These resources are to be managed efficiently and to be used effectively by planning and control by the other associate resources such as the surgeon, anesthetist, physician, and nursing staff. The scope includes a provision these critical resources. More than any other service industry, handling of emergency in the hospital is highly critical and hence detrimental to the distinctive service. The resource planning must consider the emergency requirement of the customers which are difficult to predict and control. With this backdrop, we can discuss the mission critical applications in the hospital industry.
Types of Applications
Front End Applications are developed and implemented for front end users like data entry operators, managers and other non technical users of a hospital.
Patient Database is developed to handle the queries on the existing patients and the patients treated and discharged. The queries may come from a visitor, a doctor or any other staff of the hospital.
Medical server database can contain name, addresses, telephone, etc. of all medical staff including doctors, nurses, and technicians. Holiday, work times, and locations on weekdays for contact.
Resource planning and control has important service centers in the town where support services can be obtained in emergency. These are the laboratories, the blood banks, the special clinics and the special facility centers. An online query facility to answer the number of queries on the availability, scheduling and rescheduling of the resources and the facilities. Also for judging the usage of the facilities and to put them in proper use.
Medical case history database is a Knowledge database on the case history for the guidance and research. It also monitors the effect of drugs to judge the efficacy in terms of the patients response. It analyzes the health care demand and makes planning for the health service strategy.
Back office Applications are applications are used by top management persons of a hospital and basically developed for decision support systems or special purpose systems.
The Care Applications are Manpower and personnel planning, Payroll and the employee related applications, Hospital billing and recovery, Inventory control-procurement, planning and control, Expiry date management, Financial accounting, Capital budgeting and expense control, Maintenance of the service facilities, Resource utilization and analysis.
Critical Control Applications evolve the basic standards for control and provide exception reports to the management for forward planning and control. They track Patients waiting time and service cycle, Non use of critical resources, Stock outs of the critical drugs, and the time taken to restore supply, Number of patients admitted, treated and cured, Length of the stay, cost and revenue to the hospital, New trends in the service demands and the service performance in such cases, Analysis of the delays in terms of duration and causes, Number of patients turned down or sent to the other hospitals for want of facilities-analysis and causes.
Patient Informatics
For years, medical and nursing students have been taught Florence Nightingales dictum-first, do no harm. Yet evidence from a number of sources, reported over several decades, indicate that a substantial number of patients suffer treatment-caused injuries while in the hospital. More than half of the injuries are related to use of medication. It is found that 64% were preventable.
In 1991, the Harvard medical practice study reported the results of a population-based study of iatrogenic injury in patients hospitalized in New York state in 1984. Nearly 4% of patients suffered an injury that prolonged their hospital stay or resulted in measurable disability. For NEW YORK, this equaled 98609 patients in 1984. Nearly 14 % of these injuries were fatal. If these rates are typical of the unites states, then 180000 people die each year partly as a result of iatrogenic injury , the equivalent of three jumbo-jet crashes every 2 days. When the causes are investigated, it is found that most iatrogenic injuries are due to errors and are, therefore, potentially preventable. When the causes are investigated, it is found that most iatrogenic injuries are due to errors and are, therefore, potentially preventable. For example in the Harvard medical practice study 69% of injuries were due to errors (the balance was unavoidable). Error may be defined as an unintended act (either of omission or commission) or one that does not achieve its intended outcome. Indeed, injuries are but the tip of the iceberg of the problem of errors, since most errors do not results in patient injury. For example medication errors occur in 2% to 14% of patients admitted to hospitals, but most do not results in injury. Aside from studies of medication errors, the literature on medical error is sparse, in part because most studies of iatrogenesis have focused on injuries (e.g., the Harvard medical practice study). When errors have been specifically looked for, however, the rates reported have been distressingly high. Autopsy studies have shown high rates (35% to 40%) of missed diagnoses causing death. One study of errors in a medical intensive care unit revealed an average of 1.7 errors per day per patient, of which 29 % had the potential for serious or fatal injury. Operational errors (such as failure to treat promptly or to get a follow-up culture) were found in 52% of patients in a study of children with positive urine cultures.
Autopsy studies have shown high rates (35% to 40%) of missed diagnoses causing death. One study of errors in a medical intensive care unit revealed an average of 1.7 errors per day per patient, of which 29 % had the potential for serious or fatal injury. Given the complex nature of medical practice and the multitude of interventions that each patient receives, a high error rate is perhaps not surprising. The patients in the intensive care unit study, for example were the recipients of an average of 178 activities per day. The 1.7 errors per day thus indicate that hospital personnel were functioning at a 99% level of proficiency. However a 1% failure rate is substantially higher than is tolerated in industry, particularly in hazardous fields such as aviation and nuclear power. As W. E. Deming points out (written communication, November 1987); even 99.9% may not be good enough. If we had to live with 99.9%, we would have 2 unsafe plane landings per day at O Hare, 16000 pieces of lost mail every hour, 32000 bank checks deducted from the wrong bank account every hour.
Physicians, nurses and pharmacists are trained to be careful and to function at a high level of proficiency. Indeed, they probably are among the most careful professionals in our society. It is curious, therefore, that high error rates have not stimulated more concern and efforts at error prevention. One reason may be a lack of awareness of the severity of the problem. Hospital-acquired injuries are not reported in the newspapers like jumbo-jet crashes; for the simple reason that they occur one at a time in 5000 different locations across the country. Although error rates are substantial, serious injuries due to errors are not part of the everyday experience of physicians or nurses, but are perceived as isolated and unusual events outliers. Second, most errors do no harm. Either they are intercepted or the patients defences prevent injury. But the most important reason physicians and nurses have not developed more effective methods of error prevention is that they have a great deal of difficulty in dealing with human error when it does occur.
Physicians are emotionally devastated by serious mistakes that harm or kill patients. Almost every physician who cares for patients has had that experience, usually more that once. The emotional impact is often profound, typically a mixture of fear, guilt, anger, embarrassment, and humiliation. However, as Christensen et al note, physicians are typically isolated by their emotional responses; seldom is there a process to evaluate the circumstances of a mistake and to provide support and emotional healing for the fallible physician. Thus although the individual may learn from a mistake and change practice patterns accordingly, the adjustment often takes place in a vacuum. Lessons learned are shared privately, if at all and external objective evaluation of what went wrong often does not occur. As HILFIKER points out, we see the horror of our own mistakes, yet we are given no permission to deal with their enormous emotional impact the medical profession simply has no place for its mistakes. Finally, the realities of the malpractice threat provide strong incentives against disclosure or investigation of mistakes. Even a minor error can place the physicians entire career in jeopardy if it results in a serious bad outcome. It is hardly surprising that a physician might hesitate to reveal an error to either the patient or hospital authorities or to expose a colleague to similar devastation for a single mistake.
The paradox is that although the standard of medical practice is perfection- error-free patient care- all physicians recognise that mistakes are inevitable. Most would like to examine their mistakes and learn from them. From an emotional standpoint they need the support and understanding of their colleagues and patients when they make mistakes. Yet, they are denied both insight and support by misguided concepts of infallibility and by fear: fear of embarrassment by colleagues, fear of patients reaction, and fear of litigation. Although the notion of infallibility fails the reality test, the fears are well grounded.
Work should be designed to minimise the requirements for human functions that are known to be particularly fallible, such as short-term memory and vigilance (prolonged attention). Clearly the components of work must be well delineated and understood before system redesign. Checklists, protocols, and computerised decision aids could be used more widely. Physicians should not have to rely on their memories to retrieve a laboratory test result, and nurses should not have to remember the time a medication dose is due. These are tasks that computers do much more reliably than humans. Creative ways need to be developed for making information more readily available: displaying it where it is needed, when it is needed, and in a form that permits easy access. Computerisation of the medical record, for example, would greatly facilitate bedside display of patient information, including tests and medications. LAN, WAN, PAS, PACS, and DAT- the acronyms trip off the tongue, but still most doctors ask, What is medical informatics? It presents an alluring vision. Take the all too familiar nightmare of a doctor in a busy outpatient clinic, reviewing for the first time a complicated case of a patient with heart disease and struggling with multiple sets of thick notes. The doctors wonders what colleagues have done previously, which treatments have been tried, what the most recent electrocardiogram and chest radiograph showed, and above all else, whether there is a plan. Time and energy are wasted, muddle is common, and clinical information system that presents a relevant summary of the medical record with key points highlighted, indicates the stage in the protocol for managing ischemic heart disease that has been reached, provides access to the hospitals manual of cardiac treatments, orders investigations, books a follow up visit and sends the clinic letter automatically. The doctor is smiling and able to concentrate on the patients needs. The rationale for medical informatics is that information system can provide an important part of the processes needed to deliver effective and efficient health care. Their purpose is not to replace the skills of doctors but to augment those skills and to help put the knowledge of what works into practice.
Software Impelementation
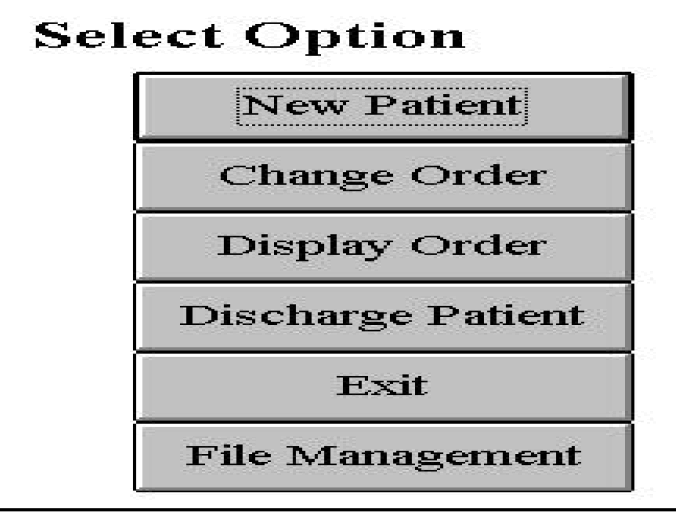
So with this background we will focus on one aspect of Use of IT in Health Services as Nursing Order Information for Nurses. This software displays relevant patient care information against time scale. One glance can update a doctor or nursing in-charge regarding the treatment status and investigations profile of many patients simultaneously, here we intend to change the old, inefficient practice of maintaining nursing register, at the same time the intention is to provide next action to be taken for nursing in-charge as well as nurses to improve information access. There can be various options like:
New Patient Information
Change Order of Medication
Display Order of Medication
Discharge Patient
File Management
This can be shown by a screen shot given in fig. 1.
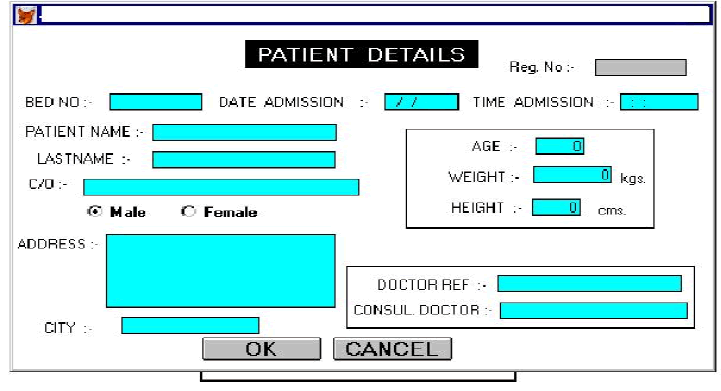
New Patient Information will have a front-end screen as shown in fig. 2 can be used to enter the patients data viz. Reg. No. , Bed No. , Date and Time of Admission, Name, Address, Age, Weight, Sex, Consulting Doctor and Doctor Reference.
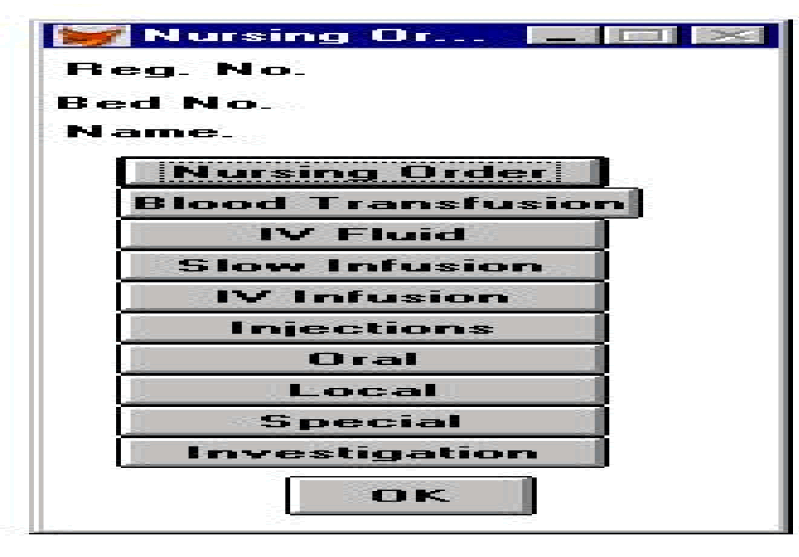
Order Screen for Doctor shown in fig. 3 can help the doctor to prescribe his nursing order by making mostly selections & typing few things. There should be numerous selections of medicines, injections, tests etc.
The doctor can call up the desired screen only from the main screen. This will save the doctors time. On the nurses part, now since the nursing orders are displayed on the screen, the clarity of information will reduce errors of misunderstanding by the nurses. With the help of this software the physician keeps control on the nursing order even when away from the patient. The screenshot of the ordering done by him is displayed as shown in fig. 3 as shown:
This software is developed in various Indian languages and is implemented and tested in the Hospitals in various cities in India successfully. The main function is that it provides the nursing actions on a time scale, so that nurses can see their next action to be taken on the screen itself. The software searches data every ten minutes from the source for updates, if any and then displays the information on the output device.
Analysing the Data
To identify the change of satisfaction level before implementing information systems and after implementing information systems (after 15 days) following data is analysed here:-
Q1. How many times you call the nurses per day ?
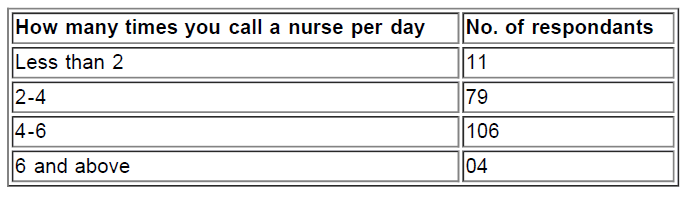
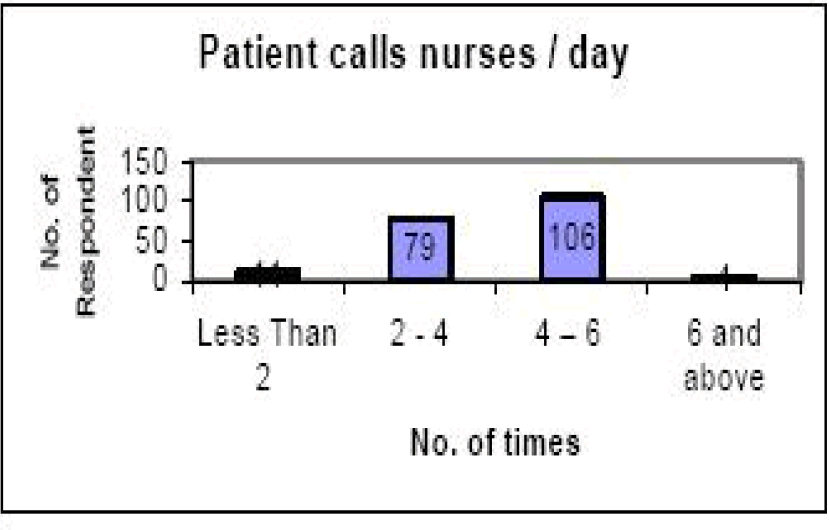
Interpretation: The data supports the findings of q.1 of the nurse section above where nurses accepts that they attend patients on the call of patient/their attendants.
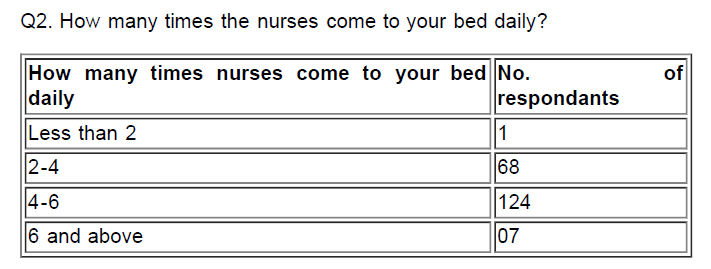
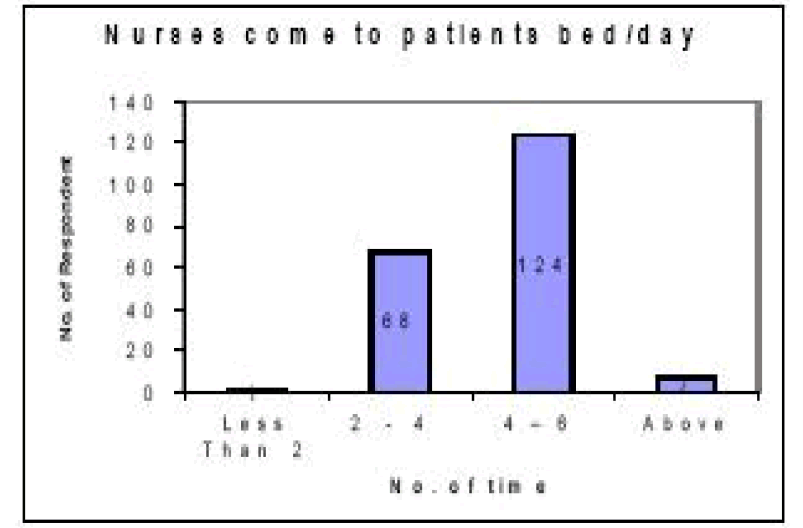
Interpretation: The data again supports of the finding about nurses work load where it was interpreted that nurses are over burdened.
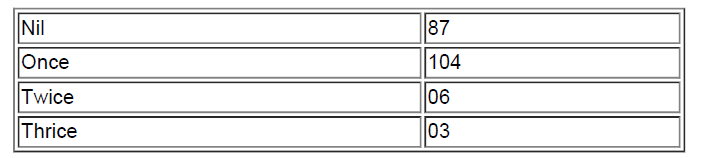
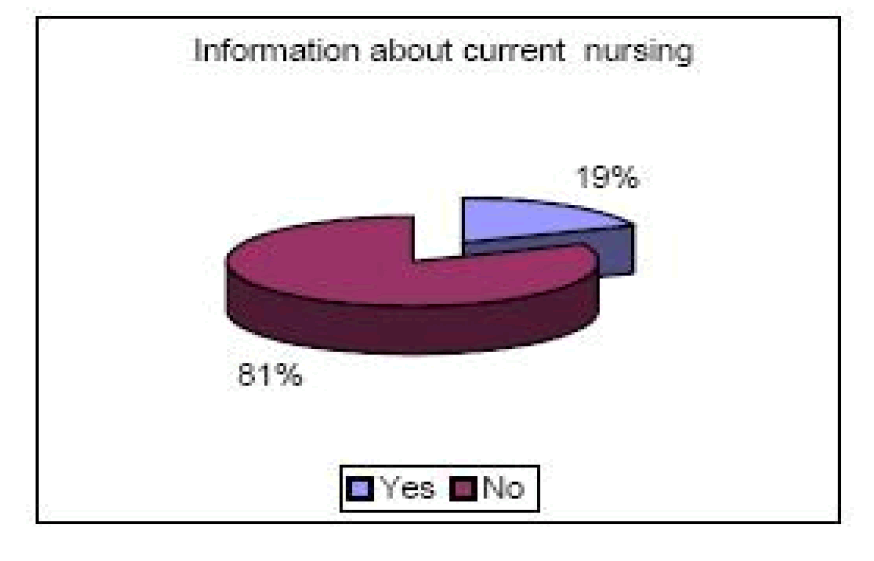
Q3. Do you know about the current nursing?

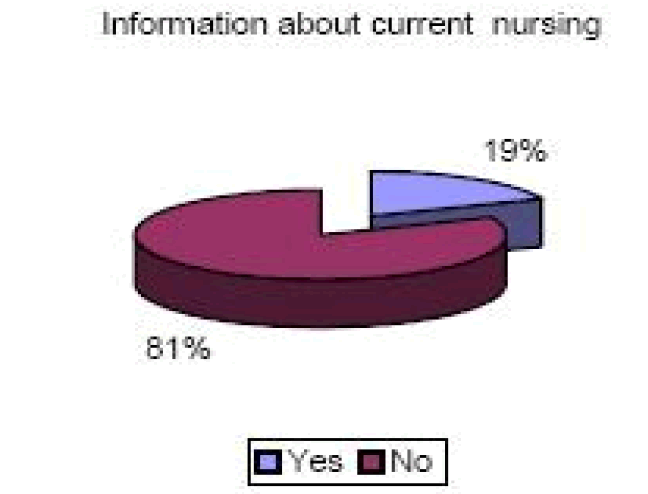
Interpretation: This shows the awareness level of patients or their attendants about nursing actions. This again reflects the need of information systems to know at least about the current nursing actions to be taken.
Q4. How many times you call the nurses after implementing Information System?
Interpretation: The number of calls for nurses is reduced to 44% because of the information systems. This justifies the aim of the research.
At the end this can be summarized that the information systems for doctors, nurses and for patients are the need of todays hospitals. These information systems can improve 21% effectiveness of the hospital services approximately.
With this Nursing Order Information software implementation and the observed results we conclude that the level of awareness has increased considerably. The readily available information has increased the transparency in the whole process and has thus helped to reduce the number of iatrogenic injuries by compelling the timely execution of any desired action to be performed by the Nurses. And along with this the load of doctor has been diversified by the software.
Copyright © 2026 Research and Reviews, All Rights Reserved